|
© Thomas Tobin
2006, 2013
The
Mare Reproductive Loss Syndrome (MRLS), the Septic Penetrating Setal
Emboli Pathogenesis thereof and Recently Reported Caterpillar Related
Abortions in Camels
Thomas Tobin, MVB, MSc, PhD, MRCVS, DABT,
Professor of Veterinary Science and Professor,
The
GraduateCenterfor Toxicology,
The
MaxwellH.Gluck
EquineResearchCenter
Universityof
Kentucky
Lexington
,Kentucky40546-0099
www.thomastobin.com
and
Dr.
Kimberly Brewer, DVM
1711 Lakefield North Court
Wellington
Fla
33414
OVERVIEW:
THE MARE REPRODUCTIVE LOSS SYNDROME (MRLS)
In three weeks around Derby Day, May 5th, 2001,
Central Kentucky
lost one third of its in utero foal crop to the Mare Reproductive
Loss Syndrome (MRLS). Total losses were estimated at $500 million. MRLS
was characterized by minimal clinical signs in affected mares,
relatively non-specific bacterial infections in aborted fetuses, and was
also associated with a very small number of highly unusual unilateral
uveitis cases. Investigations
were immediately begun to determine the cause/s of this syndrome.
Infectious causes were ruled out early. Field and epidemiological
studies linked the syndrome to a coincident epidemic of Eastern Tent
Caterpillars (ETC), suggesting a toxin driven syndrome. Numerous
candidate environmental toxins were investigated and ruled out; then,
when the seasonal ETCs became available in April of 2002, they were rapidly shown to
produce Early and Late Fetal Losses (EFL and LFL) in pregnant mares.
Working with the late fetal loss model we saw our first fetal
losses at three days after our first 50 g/day caterpillar administration.
We
immediately abandoned the toxin hypothesis and assigned a primary
abortifacient role to the bacteria; the question then became how
exposure to the caterpillars caused bacteria to enter the fetal
membranes.
Electron Micrographic (EM) studies in the summer of 2001 had
shown the ETC setae (hairs) to be barbed. We therefore considered the
possible outcomes if small numbers of barbed setal fragments penetrated
the intestinal tract, entered intestinal blood vessels, and then
re-distributed following cardiac output. Penetration
of fetal membranes by these distributing/distributed septic setal
fragments/emboli would directly introduce bacterial contaminants into
the fetus, where they would proliferate unchecked by the immature fetal
immune system. This
probabilistic model immediately explained the early and late fetal loss
events, and also the relatively rapid onset of late fetal losses, and most importantly, the
unique unilateral uveitis cases occurring in
horses of any age or sex. This
biologically unique model, identified on July 10th, 2002, we named the Septic Penetrating Setal Emboli
(SPSE) Model of MRLS and
it was immediately communicated to selected colleagues.
Replication of the LFL abortions in 2003 using a higher (100 g/day) dose
of caterpillars and a similar dose of irradiated caterpillars enabled us
to demonstrate that the LFL abortions follow a unique probabilistic
statistical model elucidated by Accelerated Failure Time analysis.
Furthermore, this model showed that the initial intensity of the
abortion response was exponentially related to the caterpillar dose; at
high doses of caterpillars exposed mares abort very rapidly, while the
caterpillars are underfoot, as had happened in Kentucky in 2001. On
the other hand, at lower doses the abortions are delayed and many
abortions occur after the caterpillars have dispersed, obscuring both
the role of the caterpillars and their relationship to the syndrome.
This highly significant probabilistic mathematical analysis underlying MRLS
was developed soon after Memorial Day, 2003.
These unusual mathematical characteristics of MRLS strongly supported our
proposed Septic Penetrating Setal Emboli model. Then, in the fall of
2003, colleagues necropsying pigs that had been dosed with ETC observed
numerous intestinal microgranulomas encasing setal fragments. These
setal fragments are septic penetrating setal fragments that did not
enter blood vessels; as such these findings provided substantial
histological evidence in direct support of our septic penetrating setal
emboli hypothesis. Similarly,
colleagues dosing rats with ETC in 2001 had observed but not
communicated their identification of similar intestinal microgranulomas
containing setal fragments, as presented here.
This simple septic penetrating setal mechanism is obviously a defensive
mechanism of the caterpillar, and likely a very ancient one. Review of
this proposed mechanism immediately suggests that other caterpillar
setae or indeed any mechanically equivalent structure should produce
similar syndromes. More
recently a syndrome closely related to MRLS named Equine Amnionitis and
Fetal Loss (EAFL) has been identified in
Australia. It is associated with
exposure to processionary caterpillars, and administration of
processionary caterpillars has been shown to abort pregnant mares. Since
then, this and apparently similar caterpillar related field and
experimental abortions have been shown to be associated with
caterpillars, including Eastern Tent Caterpillars (ETC) in Kentucky (
02, 03) and Florida (06) and other caterpillar species in Australia
(March, 05) and Florida (September, 05). Additionally,
recent reports by Volpato and Di Nardo and their colleagues (2013) make
clear that exposure to/ingestion of caterpillars by pregnant camels has
long been recognized as a cause of camel abortions in camel pastoralist
communities in the Western Sahara.
DEVELOPMENT OF THE “SEPTIC PENETRATING SETAL EMBOLI”
HYPOTHESIS
OF MRLS, 2002
The proposed septic penetrating setal emboli based pathogenesis of
MRLS, first conceived in July 2002, explains many of the unique clinical and
epidemiological characteristics of MRLS. The late term fetus is the largest mass of immunologically poorly
protected tissue in the mare; as such it is a large and highly
accessible and vulnerable target, explaining the very rapid onset of
experimental late term fetal losses. The
early fetus is a smaller target, but when accessed by a septic
penetrating setal fragment is equally vulnerable. The eye is a very
small target indeed, explaining the very small number of affected eyes. Additionally,
the uniquely unilateral nature of the eye lesions is consistent with and
in fact requires the uniquely quantal nature of the septic penetrating
setal emboli hypothesis. This hypothesis was shared on a confidential
basis with selected colleagues within hours of conception, then with a
somewhat broader group of colleagues and selected administrators the
following Monday and soon thereafter at the late July 2002 Bain Fallon Lectures,
The Gold Coast,
Australia.
SUPPORTING INFORMATION #1:THE UNIQUE MATHEMATICS OF
MRLS, 2003
The following year (May 03) more LFL abortion rate data
became available and working with Dr. Marie Gantz of the Dept. of
Statistics we showed that experimental LFL closely follows a unique
probabilistic mathematical model called Accelerated Failure Time
analysis. This unusual mathematical signature is consistent with the
unique clinical data, the probabilistic nature of the proposed septic
penetrating setal emboli hypothesis, and the unusual field epidemiology
of MRLS. As such, these
findings were rapidly written up and submitted for publication as a paper
on the toxicokinetics of MRLS (Sebastian et al., 2003). Additionally, because the septic penetrating setal emboli
hypothesis was viewed with skepticism by some of our colleagues, this first
paper was drafted avoiding a direct presentation of our underlying
septic penetrating setal emboli hypothesis. However,
US Copyright for a document describing the overall hypothesis (Copyright#TXU1111484:
2003) was registered with the Library of Congress, June 17, 2003, and a paragraph describing the SPSE
hypothesis was added to the paper prior to publication.
SUPPORTING INFORMATION #2:
IDENTIFICATION OF THE INTESTINAL MICROGRANULOMAS CONTAINING SETAL
FRAGMENTS, 2003
While this Toxicokinetic paper was under review (Fall 2003) we
learned that colleagues performing necropsies on ETC dosed
pigs had observed multiple intestinal microgranulomas in these animals,
each containing a minute central setal fragment. These setal fragments
represent septic penetrating setal fragments that have penetrated the
intestine but which did not penetrate blood vessels to become septic
penetrating setal emboli. Rather, they became encapsulated in intestinal
microgranulomas fully consistent with the first intestinal penetration step of
this proposed hypothesis. Colleagues
at the State University of New York at
Cortland kindly made similar slides available to us from some ETC dosing
experiments on pregnant rats, as presented in this communication.
SUPPORTING INFORMATION #3: LACK
OF CLINCAL SIGNS IN AFFECTED MARES
An unusual aspect of MRLS is the lack of clinical signs in affected
mares and the inability to culture bacteria from the bloodstream of MRLS
mares. The unique eye data
allowed us to estimate the actual number of circulating setal fragments
in MRLS mares. Based on
these calculations it appears that the number of setal fragments
actually distributing in an MRLS mare is very small, likely less than
ten/day in field cases. This
finding explains the lack of clinical signs in affected mares and the
apparent inability to culture bacteria from the blood of clinical and
experimental MRLS mares.
SUPPORTING INFORMATION #4:THE UNIQUE PLACENTITIS OF
MRLS
More recently, the placentitis associated with late fetal loss has
been recognized by our colleagues as pathologically unique and we
believe entirely consistent with this proposed pathogenesis of MRLS, namely the
septic penetrating setal emboli or setal hypothesis of MRLS.
2013: SUPPORTING INFORMATION #5:
CATERPILLARS RECOGNIZED AS THE CAUSE OF OTHER ABORTIONS,
INCLUDING CAMEL ABORTIONS
An immediate (July 10th, 2002
) conclusion from this proposed pathogenesis was that mechanically
and bacteriologically equivalent barbed setal fragments (or mechanically equivalent structures)
from any source should reproduce the
syndrome. As of January
2013, the world score for caterpillar related equine abortions included
Eastern Tent Caterpillars (Malacosoma Americana) from Kentucky,
Northern Michigan (02) and Florida (06), Processionary caterpillars (Ochrogaster
lunifer) in Australia (March 05), Gypsy Moth Caterpillars (Lymantria
dispar) in an experimental challenge in Kentucky (03?) and, in
September 05 in Florida, field abortions reportedly associated with
Walnut Caterpillars (Datana integerrima). Finally,
and most interestingly, there are recent reports by Volpato and
Di Nardo and their colleagues (2013) making clear that exposure to or
ingestion of
caterpillars has for long been known, and unequivocally ("everybody
knows") recognized as
a cause of abortions in camels among several groups of nomadic camel
pastoralists in the Western Sahara, consistent with an earlier report
suggesting caterpillars as a cause of abortions in camels (Bizimana,
1994).
1. THE MARE REPRODUCTIVE LOSS SYNDROME (MRLS)
During three weeks around May 5th 2001
,Central Kentucky
abruptly lost 20% to 30% of its in-place foal crop. Of
foals conceived in the spring 2001, about 2000 were lost, the so-called
Early Fetal Losses (EFLs). Of
foals conceived the previous spring and then close to term, at least 600
were lost, the so-called Late Fetal Losses (LFLs). Based
on these overwhelming reproductive losses, the syndrome was named the
Mare Reproductive Loss Syndrome, or MRLS. The
total economic loss for the 2001 MRLS season to
Kentuckyand the breeding and racing industry was initially estimated at greater
than $330 million. MRLS, as
such, had never previously been recognized.
|
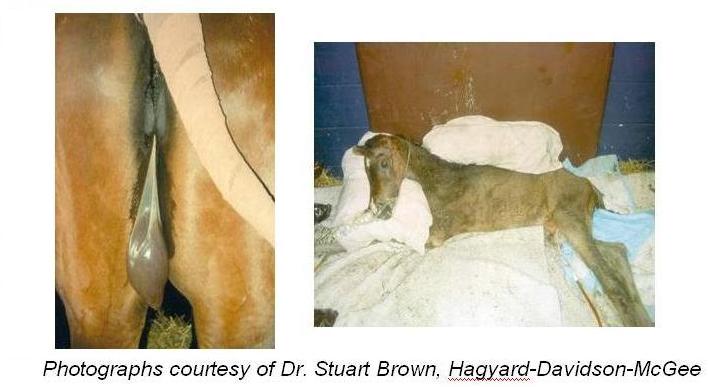
Figure 1.Early (left panel) and late Fetal Losses (right panel) of MRLS.
|
2. THE ANCILLARY SYNDROMES
Soon three ancillary syndromes were recognized and included in the case definition. These syndromes included about 60 coincident cases of fibrinous pericarditis
(epicarditis? Fig 2.), and a slightly smaller number of what can only be described as a unique unilateral panopthalmitis, along with three cases of Actinobacillus encephalitis. These ancillary syndromes, occurring in both male and female horses, were included in the case definition of MRLS.
|
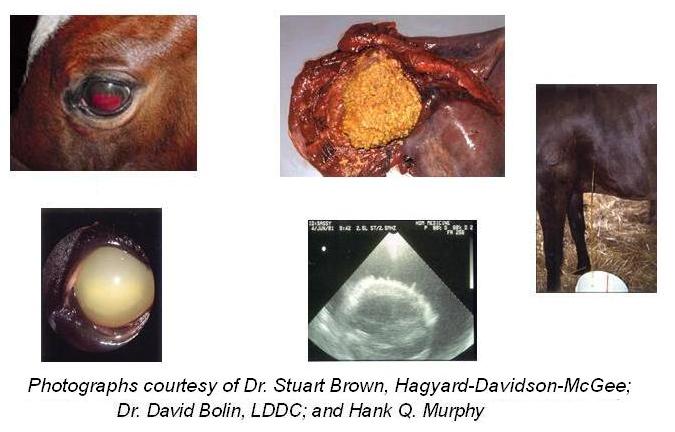
Figure 2. The Associated Unilateral Uveitis (left) and Pericarditis (right) Cases:
|
3. FIRST OBSERVATIONS:EARLY FETAL LOSS (EFL) OBSERVATIONS
MRLS was first identified on
April the 26th 2001
by Dr. Thomas Little, who on that day observed an unusual number of in
utero deaths in 60 day-old fetuses in clinically normal mares that he was ultrasounding for sex
determination. These early
fetal losses were followed by an overwhelming sequence of early and late
fetal losses and, somewhat later, the coincident pericarditis, uveitis
and encephalitis syndromes, occurring in very much smaller numbers in
horses of all ages and sexes were identified.
4. THE PATHOLOGY OF THE LATE TERM FETUSES
The abortions, and particularly the late-term abortions, showed
characteristic pathology. There
were an increased number of "red bag" presentations with weak
and stillborn foals. Necropsy
evaluation of aborted foals showed inflammation of the amnion, the
umbilicus [funisitis], and the fetal lungs. Bacterial isolates included
a high proportion of alpha streptococci, actinobacillus and many other
isolates, including Serratia. The Early and Late abortion syndromes
peaked on about May 5th 2001, Derby Day, and were essentially over by the end
of May.
5. THE EXCLUSION OF INFECTIOUS CAUSES
Within the first week extensive bacteriological and virological
work, the essential lack of clinical symptoms in affected mares, as well
as the essentially simultaneous appearance of the syndrome across the
Bluegrass
largely excluded an infectious cause. Work
then focused on identifying an environmental toxin or agent as the cause
of the syndrome.
6. THE INITIAL TOXICOLOGICAL EVALUATIONS
Within two weeks toxicological investigations had ruled out
nitrate/nitrite toxicity; work then focused on toxins with reproductive
associations; additionally, because of a coincident unusually intense
infestation (plague?) of Eastern Tent Caterpillar (ETC, Malacosoma
americana), the possibility of an association of the syndrome with
the black cherry tree/Eastern Tent Caterpillar biological system was
very carefully evaluated.
7. CLUE #1: THE TIME
AND PLACE ASSOCIATIONS WITH THE CATERPILLAR
Within three weeks preliminary field
investigations by Dr. Jimmy Henning of the Univ. of Kentucky College of
Agriculture pointed to a close association between the presence of black
cherry trees/Eastern Tent Caterpillars and MRLS. Additionally,
preliminary toxicological evaluations suggested increased concentrations
of cyanide in the hearts of some LFL fetuses. The
association of MRLS with presence of the caterpillar was later confirmed
by a rigorous epidemiological survey by Dr. Roberta Dwyer of the
Gluck
Equine Research Center and her
associates (Dwyer et al., 2003).
These
early findings were critically important, because they focused attention
squarely on the caterpillars, which were present in enormous numbers at
many locations in central
Kentucky at the time of the MRLS outbreak.
|

|
Figure 3a.The large numbers of caterpillars during the
outbreak.Here they cover a water bucket.
Figure
3b.The Eastern Tent Caterpillar
 |
8. CLUE #2: THE BARBED SETAE
ON THE CATERPILLARS
The early focus on the caterpillar led
Mrs. Pat Van Meter and me to examine them under the Electron
Microscope at about the time of the 2001 outbreak (Fig 3c)). We
noted, in passing, the barbed nature of the very fine setae that
cover the exterior of the caterpillar and we also noted that in
some caterpillar species these setae are venomous and extremely
effective offensive weapons. Although
not specifically recognized as such at the time, these were
critically important observations.
|
Figure 3c.Barbed setae
 |
|
9. THE
ENVIRONMENTAL TOXIN HYPOTHESIS
The search for the cause of MRLS at first focused on candidate
environmental toxins, at least in part because Eastern Tent Caterpillars
were unavailable, being out of season. Over
the next nine months rigorous evaluation of the possible roles of plant
estrogens, mycotoxins, ergot alkaloids and Hemlock alkaloids failed to
produce any evidence suggestive of a role in MRLS. The
possible role of cyanide in MRLS was very carefully examined because of
the close association of the Eastern Tent Caterpillar with cyanogenic
Black Cherry trees. Rigorous
experimental evaluations failed to show any association between cyanide
and MRLS (Camargo et al., 2002; Dirikolu et al., 2003). Additionally,
vigorous efforts to induce abortions with a variety of toxins, including
cyanide and mandelonitrile (an intermediate in the release of cyanide
from cherry leaves) and a number of other candidate toxins failed, each
and all.
10. SPRING 2002: RETURN OF THE CATERPILLARS AND
EXPERIMENTAL
AND FIELD ABORTIONS
Return of the Eastern Tent caterpillar in spring 2002 showed that
exposure of early pregnant mares to Eastern Tent Caterpillars rapidly produced
early and late fetal losses, and the abortions closely resembled field
MRLS (Webb et al., 2004). By May 2002 it was
therefore clear that MRLS was very closely associated with the
Caterpillar itself; the question then became how the caterpillar, or
factors associated with the caterpillar, produced the abortions.
11. CLUE #3: RAPID ABORTIONS IN THE 2002 LATE FETAL LOSS
EXPERIMENT:THE BACTERIAL ABORTION THEORY
Towards the end of the 2002 ETC season we administered 50 g/day of
Northern Michigan ETC by intubation to Late Term pregnant mares. The
first abortions occurred very rapidly, within 72 hours, suggesting to us
that the primary driving event in the abortions was most likely
bacterial proliferation in the fetus and/or fetal membranes. We
therefore abandoned the toxin hypothesis and review of this changed
etiology for the abortions and the well established tissue penetrating
capabilities of barbed caterpillar setal fragments led us virtually
immediately (July 10th, 2002) to the Setal/Septic Penetrating
Setal Emboli Hypothesis of MRLS.
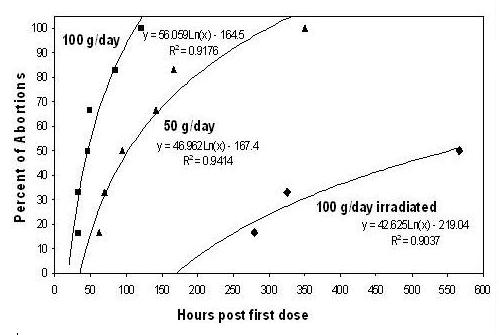
Figure
4. CLUE #2:
Very
rapid time course of abortions following dosing of mares with 50 (02)
and 100 (03, nonirradiated or radiated) grams of Eastern Tent
Caterpillars (ETCs) per day for 10 days. The solid lines are
the best fit regression for the data points. The calculated x-axis
intercepts (apparent lag times) are 20 (100g), 37 (50g), and 193
hours (100g irradiated) after the first dose of ETCs.
|
12. CLUE #3,
2002: BARBED SETAL FRAGMENTS: THE
SEPTIC
PENETRATING SETAL EMBOLI (SPSE) HYPOTHESIS OF MRLS
Considering the barbed setae of the caterpillars, we proposed that
MRLS results from movement driven intestinal penetration by barbed setal
fragments, with their associated bacteria (septic penetrating setae),
followed by blood vessel penetration and hematogenous redistribution of
a proportion of these setal fragments, now forming "Septic Penetrating Setal Emboli" (Tobin et al., 2003, 2004). Systemic
distribution of such embolic setal fragments would follow cardiac
output, as is well described and understood with regard to drug
distribution. These septic setal fragments would then randomly lodge in
distant tissues, and their retained structurally based ability to
penetrate moving tissues would allow them to distribute their bacterial
contaminants in any moving distant tissue in which they lodged. Significant
pathology would result only if the penetrated tissue was poorly
protected immunologically. A
reduced local immune response was, and is, a critical part of the
proposed pathogenesis.
Figure 5.Schematic Construct of Intestinal wall and Intestinal Venule Penetration by Barbed Setal Fragment.
 |
13. THE CRITICAL ROLE OF
TARGET TISSUE MASS AND
REDUCED
IMMUNE RESPONSES
The late term fetus is the largest mass of
immunologically poorly protected tissue in the mare. As
such, it is a large and vulnerable target, explaining the unusually
rapid onset of our experimental late term fetal losses. The
early fetus is a much smaller target and therefore less likely to be
"hit,"
but an equally vulnerable target once hit. The
eye is a very small target indeed, explaining the very small number of
affected eyes. Additionally,
the uniquely unilateral nature of the uveitis cases is entirely
consistent with and requires the discrete, quantal, and very small number,
nature of the proposed triggering septic penetrating setal emboli
insults.
13.1. INITIAL RECEPTION OF THE SPSE / MRLS HYPOTHESIS
This "septic penetrating setal emboli" hypothesis as a
proposed mechanism for MRLS was conceived on or about July 10th 2002. It was communicated to selected colleagues within hours and within
days to selected administrators; it would be fair to say that its
reception was unenthusiastic, to the point that its presentation at many
levels was perceived as being discouraged.
14. THE CLINICAL SIGNATURES OF THIS
PROBABILISTIC MECHANISM
14.1. THE EFFECT OF TARGET
SIZE
This proposed pathogenesis depends on the
statistical probability of a distant tissue penetration event occurring
for any given poorly immune protected tissue. As set forth above, it was immediately
clinically obvious that the
actual size (target size) of the immunologically poorly protected target
would influence the probability and therefore the rate at which any
clinically effective septic setal “hit” (or clinically observable
result) would occur. These
factors immediately explained the rapid onset of the LFL experimental
abortions, given the large size of the Late Fetus, which on a weight
basis receives at least 15% of the mare’s cardiac output. The early term fetus is much
smaller and receives proportionally
much less cardiac output. The early term fetus is therefore
statistically much less likely to receive a setal “hit,” thereby
explaining the much slower rate of occurrence of the EFL experimental
abortions. Indeed, very
early fetuses were perceived as being protected from MRLS, likely a
result of their very small target size. The single eye is a very small target indeed, explaining the
relative rarity of the single eye events and the complete lack of any
double eye events. We were
soon, however, to be presented with additional and very compelling
statistical evidence of the probabilistic mathematics underlying MRLS,
namely a unique mathematical signature called Accelerated Failure Time
(AFT).
|
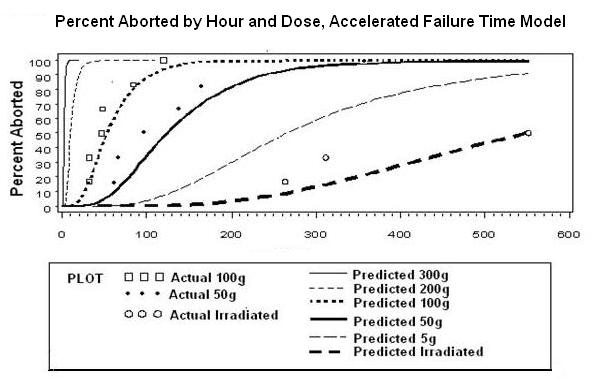
Figure 6. The Mathematical model of MRLS -- Actual abortion rates following dosing with Eastern Tent
Caterpillars |
 |
|
Accelerated
Failure Time (AFT) analysis of MRLS
Assumed
that time until abortion has a log-normal distribution a
survival model that well fits the data is an Accelerated
Failure Time Model. The model takes the form:

This
model includes an intercept term (β0)
and an error term (σεi). Ti is
the time that abortion occurs for individual i, and
β1 through
βk are
coefficients for covariates that might affect abortion time.
|
14.2. THE UNUSUAL
PROBABILISTIC MATHEMATICS UNDERLYING
MRLS:ACCELERATED FAILURE TIME ANALYSIS
Further evidence for the unique
probabilistic mathematics underlying MRLS became apparent as follows. On Memorial Day weekend of 2003 we
plotted
the
individual time courses of each of the 2002 and 2003 LFL experiments (Figure 4). The
plotted time courses of the three individual sets of MRLS
abortions in Figure 4 yielded a clear cut family of time course curves. Each
curve clearly fit a smoothly defined exponential rate from the first to
the last abortion; however, and most
unusually, each curve appeared to commence after a specified “lag
time,” and this lag time appeared to be related to the rate at which the
abortions occurred. We took
Figure 4 to Dr. Marie Gantz of the Dept of Statistics,
suggesting that we had half of the equation for MRLS, and requesting
that she provide a factor describing the lag times and we would have the
complete equation for MRLS. Dr.
Gantz pulled the required equation "off the shelf," a probabilistic
mathematical analysis called Accelerated Failure Time analysis (Fig 6). As set forth in Figure
6, the time course of MRLS LFL abortions closely follows this very
unusual probabilistic
mathematical model, entirely consistent with the probabilistic nature of
our proposed Septic Penetrating Setal Emboli model/hypothesis of MRLS
(Figs 4 and 6, P: <.0001 .0052 <.0001).
In lay terms, what this model
says is that it is the rate at which the setal distribution events occur
that determines the speed of onset of an MRLS event. If exposure to caterpillars is high, and the rate of setal
penetration/ distribution events is high, then the lag time is minimal
and the onset of occurrence of MRLS abortions is very rapid. On the other hand, if exposure to
the caterpillars is low, then the
rate of setal penetration (or entry into affected tissues) is low, the lag
time is long and the onset of the first MRLS event is much slower,
taking days to
weeks or longer, as set forth in Fig 6 above.
14.3. THE
EXPONENTIAL DOSE / TIME RESPONSE
RELATIONSHIP FOR MRLS
The second important mathematical
characteristic of this type of mechanism is that the initial intensity of the
response, in this case the rate at which the abortions occur, is
exponentially related the dose. Thus when exposure to the caterpillars
is very high, the lag time is very short, the abortions onset very
rapidly and are closely linked in time and place to the presence of the
caterpillars, as occurred in Kentucky in 2001, and which constituted clue
#1, above.
On
the other hand, when exposure to the caterpillars is low, the onset of
the abortions is delayed, their number is greatly reduced, and the
delayed abortions may occur out of phase with the presence of the
caterpillars. Additionally,
horses in
Kentucky are unlikely to be exposed to caterpillars for more than the short ETC
caterpillar migration season, about two weeks or so in
Kentucky. These unusual
characteristics of the Kentucky caterpillar driven abortions explain
both the exceptional intensity of the 2001 Kentucky ETC related abortion
storm and the fact that these abortions, although previously identified
as a discrete unexplained class of abortions, had never previously been
recognized as being related to (or caused by) the caterpillars.
In sum, these data show that
experimental and field cases of MRLS follow a virtually unique
probabilistic mathematical model called Accelerated Failure Time
analysis, which analysis is entirely consistent with the Septic
Penetrating Setal Emboli hypothesis and our proposed underlying
probabilistic mathematics of MRLS (Fig 6). These
findings in the summer of 2003 enabled us to submit for publication our
first formal toxokinetic/statistical analysis of MRLS (Sebastian et al.,
2003) and then to add,
while this manuscript was in press, a summary description of its septic
penetration setal emboli pathogenesis. Soon thereafter, this
publication was followed by the
full septic penetrating setal emboli hypothesis paper (Tobin et al.,
2004).
15. Fall O3: IDENTIFICATION OF INTESTINAL
MICROGRANULOMAS
CONTAINING SETAL FRAGMENTS
Figure 5 is a construct from our
2004 paper designed to communicate our visualization of blood vessel
penetration by a septic penetrating setal fragment. What
Fig 5 does not address is what happens to the many septic penetrating
setal fragments (SPSF) that enter the intestinal tract and do not enter a blood
vessel. Our hypothesis might
suggest that at least some if not all of these SPSF should work their
way through the intestine to its peritoneal surface and cause
peritonitis, which we were fully aware was not occurring. This
question was the next MRLS conundrum to be answered.
In we understand the late
summer of 2003 a colleague working on a pig model of MRLS necropsied
some pigs which had been dosed for several weeks with ETC. Necropsy of these ETC dosed pigs showed evidence of a very large
number of intestinal setal penetrations in the form of microgranulomas
containing setal fragments in the intestinal tract, fully consistent
with our setal hypothesis of MRLS. Discussing
these rumored findings with another colleague, Dr. Terry Fitzgerald of
Cortland University, he noted that they had made similar observations on ETC-dosed rats
(Fig 7), which slides he immediately shared.
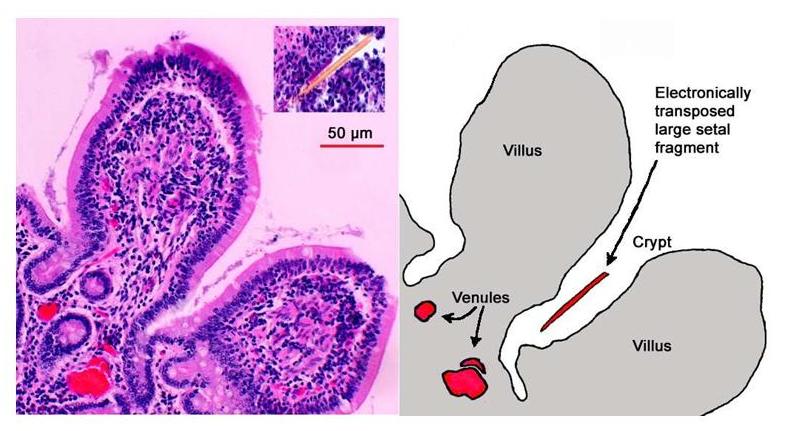
These setal microgranulomas
are interesting, because it is the microgranulomas, small enough in and
of themselves, which had caught the attention of the pathologists. In the center of each of these microgranulomas
was a much smaller
setal fragment. These are,
of course, our postulated “septic penetrating setal fragments”, that
drive MRLS, each caught and immobilized in a little connective tissue
microgranuloma capsule and presumably being slowly degraded. In any event, they are no longer “penetrating” and present
little or no further risk to the animal [or to us]. And
this, of course, is presumably how our intestinal tracts protect us from
having small barbed fragments fully penetrate our intestinal tracts and
induce peritonitis, presumably an anciently evolved digestive tract
protective mechanism. The answer to our intestinal penetration conundrum
is that the barbed penetrating fragments are isolated and walled off in connective tissue
capsules, and that effectively ends their penetrating
ability.
|
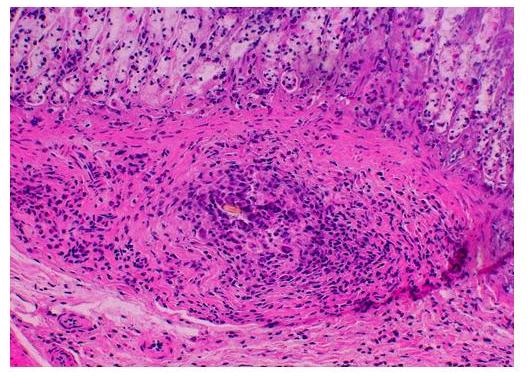
Figure 7.Intestinal Microgranuloma in an ETC dosed Rat containing an ETC Setal Fragment at its Center. Courtesy of Dr. Terry Fitzgerald and Colleagues, Cortland University, Cortland, New York.
|
16. SUPPORTING
INFORMATION:THE PERICARDITIS CASES
The pericarditis cases
are also best explained by the septic penetrating setal emboli
hypothesis. Of all tissues in the body, the contracting heart is
one through which one might expect septic penetrating setal emboli to
migrate/be driven fastest. The central role of the heart in the
circulatory system and its ongoing contractile activity may suggest that
at least 50% of setal fragments entering cardiac muscle will wind up in
the pericardial fluid. Bacteria cultured from the
pericarditis cases are those associated with MRLS, although no bacteria
were cultured from some pericarditis cases. This may suggest loss of
septic contaminants during passage of the septic material through the
cardiac musculature. The pericarditis cases are clearly most consistent
with and best explained by the septic penetrating setal emboli
hypothesis.
There is an interesting contrast between the potential outcomes of
intestinal and cardiac tissue penetration by septic penetrating setal
fragments. In the intestine, penetrating setal fragments are
rapidly “walled off” and thereby neutralized. This is
presumably an ancient intestinal defensive strategy designed to prevent
the potentially lethal outcome of peritonitis resulting from intestinal penetration
by barbed structures. Given the importance of preventing setal
penetration, it seems likely that this local “walling off” process
is accompanied by a reflex local reduction in intestinal contractility
in the affected area. On the other hand, such a strategy is not
available in the heart, where fragment movement through cardiac tissue
would presumably be much faster than through the intestinal wall and a
local reduction or cessation in contractility is a much less viable option.
17. SUPPORTING
INFORMATION: LACK OF CLINICAL
SIGNS
IN AFFECTED MARES:
An unusual aspect of MRLS was the lack of clinical signs in
affected mares and the failure to culture bacteria from the bloodstream
of MRLS mares.The unique
eye data allowed us to estimate the number of circulating setal
fragments in MRLS mares.It
appears that the number of setal fragments actually distributing in an
MRLS mare is very small, likely less that ten/day in field cases.This finding explains the essentially complete lack of clinical
signs in affected mares and the practical inability to culture bacteria
from the blood of clinical and experimental MRLS mares. In lay terms, in MRLS at least, there are simply too few setal
fragments circulating to produce an observable clinical response in the
mare herself.
18.
SUPPORTING
INFORMATION:
UNIQUE
PLACENTITIS OF MRLS:
More recently, the placentitis
associated with MRLS has been formally recognized by pathologists as
unique and clearly distinguishable from the classic and well described
ascending and hematogenous placentites, and also, we believe, fully
consistent with the unique SPSE mechanism underlying MRLS.
19. SUPPORTING INFORMATION: OTHER
CATERPILLAR DRIVEN
ABORTION EVENTS
An obvious and early prediction from this
proposed pathogenesis is that mechanically and bacteriologically equivalent barbed setal
fragments or analogous structures from any source should
reproduce the syndrome. As of January 2013, the world score for
caterpillar related abortions is, to our knowledge, as follows:
19.1.
KENTUCKY
Caterpillars have produced
numerous field abortions, MRLS in central Kentucky and
adjacent states (2002, 03) and in
Florida (2006). Also, Eastern
Tent Caterpillars from Kentucky and Northern Michigan
have been shown to be fully abortigenic in experimental situations.
In a challenge experiment in Kentucky, reported in 2004, one of four
pregnant mares exposed to Gypsy Moth Caterpillars aborted, although we
must note that the investigators chose to distinguish between this
single "GMC" related abortion and classic MRLS abortions.
19.2.
FLORIDA AND NEW JERSEY, 2006
In Florida, one of two pregnant mares exposed to high densities of Walnut
Caterpillars (Datana integerrima) aborted within one week, and
the second aborted three months later.
19.3.
AUSTRALIA, 2005
Processionary caterpillars (Ochrogaster
lunifer) were seen in association with field abortions in the Australian
Hunter Valley area (March 2005), and soon thereafter (August
2006) these caterpillars were
reported to be abortigenic in experimental tests. In
point of fact, the principal investigator in this matter was reportedly at first
reluctant to consider the possibility of caterpillar
involvement in these equine abortions. Following the suggestion of
an Australian horse farmer who had suffered significant abortion related
losses, the Australian investigator contacted our research group and
our suggested approach to the described abortion matter was unequivocal.
In our opinion,
the described syndrome was remarkably similar to MRLS, and as such, our
recommendation was, caterpillar experiments first, any and all other
experimental approaches, second. The suggested caterpillar
administration experiments were performed, and the caterpillar
administrations rapidly reproduced abortions. This syndrome, which the
Australians named
Equine Abortion and Fetal Loss (EAFL) is now recognized as being closely
related to and broadly similar to MRLS (Cawdell-Smith et al., 2012;
Todhunter, et al., 2009).
19.5. AFRICA, 2013, CATERPILLARS AND CAMEL ABORTIONS
It
is said there is nothing new under the Sun. Just recently,
researchers investigating the causes of abortions in camels reported that the Sahrawi (literally “people of the desert”) of the
north-western Sahara have long known of the association between
caterpillar ingestion and camel abortion (Volpato
et al., 2013). Though mentioned as a possible cause of camel abortions
by Bizimana in 1994, African caterpillars
have until now received little or no recognition by the scientific
community as abortifacients. The Sahrawi pastoralists are nomadic people who are dependent on camels
for their livelihood. Among
these cultures, it has long been traditional knowledge that a
caterpillar-borne reproductive loss syndrome exists. The Sahrawi people call this “duda,”
which is an Arabic name
for “caterpillar.” Duda
in camels presents many similarities to Mare Reproductive Loss Syndrome
(MRLS), suggesting a similar pathogenesis of the disease.
Caterpillars affecting mares and camels are both of the family Lasiocampidae.
The
caterpillar of MRLS (the Eastern Tent Caterpillar) is a hairy caterpillar
with barbed setae. The
caterpillar affecting Sahara
camels is known by the Sahrawi as shedbera,
and is described as a hairy caterpillar. Unfortunately because of the absence of an identified adult moth, the exact species of the Lasiocampidae caterpillar has yet to
be classified. Family
Lasicampidae larva are
generally densely hairy, feed on foliage from trees, and may build
communal tents that contain the caterpillar’s hairs and setae.
Female moths of these species lay a large number of eggs which,
if the environmental conditions are favorable, may lead to outbreaks of the
caterpillars.
Both Duda and MRLS outbreaks
are associated with large numbers of caterpillars in the environment.
When conditions are such, both horses and camels are likely
to ingest caterpillars while foraging. With Duda, the caterpillars are associated with Acacia
trees which Western Sahara camels feed on, as these trees may be
the only green pasture available. In
the
US, MRLS has been associated with environmental conditions that cause
greatly increased numbers of Eastern Tent Caterpillars in trees and
pastures where mares graze. Sahrawi
pastoralists differentiate duda as the cause of abortions in camels from
other causes based on their sudden and episodic patterns of abortion
storms associated with an abundance of shedbera caterpillars on Acacia foliage.
Like MRLS, abortion is the
primary clinical sign of Duda. The clinical signs associated with
Duda
include, in pregnant camels, abortions and uterine prolapse. Calves that are born with
Duda show weakness, red eyes, hair
falling out, astasis and incoordination, joint effusion, swelling
of lymph nodes, and diarrhea. Sahrawi
people are clear that duda is “born
with the calf”, meaning it is not caused by an external agent
after birth. These clinical
signs of duda share similarities with the clinical signs and
presentations of MRLS. Adult
camels who are not pregnant do not show clinical signs of duda, even
when ingesting the caterpillars, again similar to MRLS.
Sahrawi herders are well aware that
it is difficult for them to prevent duda, as the only means of
prevention of this syndrome would be to stop the ingestion of foliage. As
caterpillars may outbreak suddenly on the main foraging source for
camels, it is difficult for the herders to prevent ingestion of
caterpillars by grazing camels. The Sahrawi people also do not have an effective treatment for
weak affected calves born during a duda outbreak, and most of the
affected calves die. Photographs
of the duda caterpillar reveal
a remarkable similarity to the Eastern Tent Caterpillar.
Eastern Tent
Caterpillar |

Duda Caterpillar among the thorns of the Acacia
tree. (Volpato
et al., 2013) |
20. CONCLUSIONS, JANUARY 2013
We believe that only satisfactory
hypothesis offered to date to explain the unique constellation of clinical
syndromes that comprise MRLS
1. the etiology of each of the four MRLS syndromes
2. the unique
probabilistic mathematics underlying MRLS
3. the unique epidemiological presentation
4. the unique pathogenesis
5. the gross histopathological and bacteriological characteristics of
MRLS
6. the predicted and similar now-emerging caterpillar-related abortions in
horses and most recently in camels
is the Setal/Septic
Penetrating Setal Emboli hypothesis of MRLS.
We also respectfully
note that this hypothesis is without precedent in the biomedical
literature.
A
detailed presentation of this hypothesis is available for viewing in a
web slide show
(Tobin 2005) which was first presented at the July 2002 Bain-Fallon symposium in Gold
Coast,
Australia.
While the presentation has
since been expanded and updated, it retains substantial portions of the
first public presentation of the Septic Penetrating Setal Emboli Hypothesis of MRLS made in Australia
in 2002.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
REFERENCES
Adkins, P. (2005) Tracking the source of mare reproductive
loss syndrome. Equus, January, pp 46-9.
Bizimana, N. (1994) Traditional
Veterinary Practice in
Africa. Deutsche Gesellschaft fur Technische Zusammernarbeit.
pp 348-9.
Camargo, F., Dirikolu, L, Sebastian, M., Hughes, C., Crutchfield, J.,
Harkins, J.D., . Boyles, J., Troppmann, A., McDowell, K., Harrison, L.,
Tobin, T. (2002). The toxicokinetics of cyanide and mandelonitrile in
the horse and their relevance to the Mare Reproductive Loss
Syndrome. Proc 4th International Conference of Racing Analysts
and Veterinarians Orlando, FL.
Cawdell-Smith AJ, Todhunter KH, Anderson ST, Perkins NR,
Bryden WL.(2012) Equine amnionitis and fetal loss:
mare abortion following experimental exposure to Processionary
caterpillars (Ochrogaster lunifer). Equine
Vet J.44(3):282-8.
doi:
10.1111/j.2042-3306.2011.00424.x. Epub 2011 Aug 5.
Dirikolu L, Hughes C, Harkins D, Boyles J, Bosken J, Lehner F, Troppmann A, McDowell K, Tobin T, Sebastian MM, Harrison L, Crutchfield J, Baskin SI, Fitzgerald TD. (2003) The toxicokinetics of cyanide and mandelonitrile in the horse and their relevance to the mare reproductive loss syndrome.
Toxicol Mech Methods. 13(3):199-211.
Dwyer, R.M., L.P. Garber, J.L.
Traub-Dargatz, B.J. Meade, D. Powell, M.P. Pavlick and A.J. Kane. (2003).
Case-control study of factors associated with excessive proportions of
early fetal losses associated with Mare Reproductive Loss Syndrome in
central Kentucky during 2001. J. Am. Vet. Med. Assoc. 222:
613-619.
Neundorf, F. (2007) Caterpillars are aborting our
mares. Australian Performance Horse, January, pp 56-8
Sebastian M, Gantz M, Tobin T, Harkins J, Bosken J, Hughes C, Harrison
L, Bernard WV, Richter D and Fitzgerald TD. (2003) The Mare Reproductive Loss
Syndrome and the eastern tent caterpillar: A toxicokinetic/statistical
analysis with clinical, epidemiologic, and mechanistic implications. Vet
Ther,4(4):324-339.
Tobin, T. (2002) MRLS and associated syndromes: toxicological
hypotheses. Proceedings of the First Workshop on Mare
Reproductive Loss Syndrome, eds Powell, DG, Troppman, A., Tobin, T.,
University of Kentucky Agricultural Experiment Station. Lexington,
Kentucky, p 75.
Tobin T, Harkins JD, VanMeter PW, Fuller TA: (2004) The Mare Reproductive Loss
Syndrome and the Eastern Tent Caterpillar II: A Toxicokinetic/Clinical
Evaluation and a Proposed Pathogenesis: Septic Penetrating Setae.Int. J
Applied Res in Vet Med, 2(2):142-158. http://www.jarvm.com/articles/Vol2Iss2/TOBINJARVMVol2No2.pdf
Tobin, T (2005) Mare reproductive
loss syndrome (MRLS) and the eastern tent caterpillar (ETC): a
toxicological / clinical investigation and a proposed pathogenesis;
septic penetrating setae. Available for viewing on-line as a powerpoint
presentation at http://thomastobin.com/mrlspp.htm
Todhunter KH, Perkins NR, Wylie RM, Chicken C, Blishen AJ, Racklyeft DJ, Muscatello G, Wilson MC, Adams PL, Gilkerson JR, Bryden WL, Begg AP.
(2009) Equine amnionitis and fetal loss: the case definition for an unrecognised cause of abortion in mares.
Aust Vet J. 87(1):35-8.
Volpato G, Di Nardo A, Rossi D,
Saleh SM, Broglia A (2013) 'Everybody knows', but the rest
of the world: the case of a caterpillar-borne reproductive loss syndrome
in dromedary camels observed by Sahrawi pastoralists of Western Sahara.Journal of Ethnobiology and Ethnomedicine.9(5)
(10
January 2013) http://www.ethnobiomed.com/content/pdf/1746-4269-9-5.pdf
Webb, B.A., W.E. Barney, D.L. Dahlman,
S.N. DeBorde, C. Weer, N.M. Williams, J.M. Donahue and K.J.
McDowell. (2004). Eastern tent caterpillars (Malacosoma americanum)
cause Mare Reproductive Loss Syndrome. J. Insect Physiol.
50:185-193.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
FURTHER
READING
1. Proceedings of the First Workshop on Mare Reproductive Loss Syndrome
on the Web: http://www.ca.uky.edu/agc/pubs/sr/sr2003-1/sr2003-1.htm.
A one-page summary of the hypothesis is presented on page 75.
2. For more on MRLS – including caterpillar control, disease
prevention, additional research and archives – go to www.uky.edu/ag/vetscience/mrls/index.htm.
3. A complete listing of scientific articles addressing MRLS and
published by the Tobin research group is located at http://equinetoxicology.com/mrlspubs.htm.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
SUPPORT CREDITS
From the Equine Pharmacology, Therapeutics and Toxicology Program of the
Maxwell
H.
Gluck
Equine
Research
Center,
University
of Kentucky,
Lexington,
KY.
This research was supported by grants from the USDA Agriculture Research
Service Specific Cooperative Agreement #58-6401-2-0025 for Forage-Animal
Production Research, the Kentucky Department of Agriculture, the
Kentucky Thoroughbred Association Foundation, the Horsemen’s
Benevolent and Protection Association, and Mrs. John Hay Whitney.
|